humana pharmacy fax form
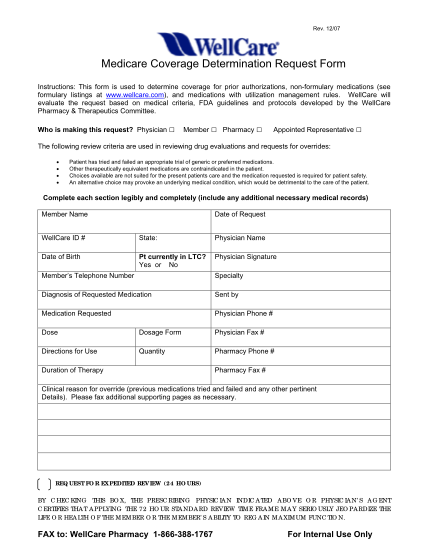
Physician fax form patient information member id (found on humana id card) gender date of birth first name male / / - female m.i. last name street number street name apt/suite # city state zip code phone number - allergies: - no known peanuts...
FILL NOW