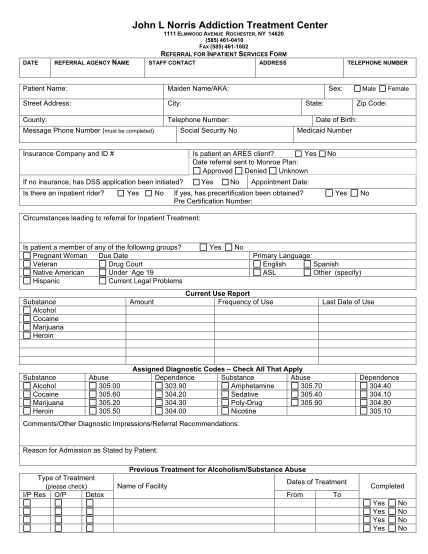
treatment inpatient form
John l norris addiction treatment center 1 elmwood avenue rochester, ny 14620 (585) 461-0410 fax (585) 461-1602 referral for inpatient services form date referral agency name staff contact address patient name: maiden name/aka: street address:...
FILL NOW