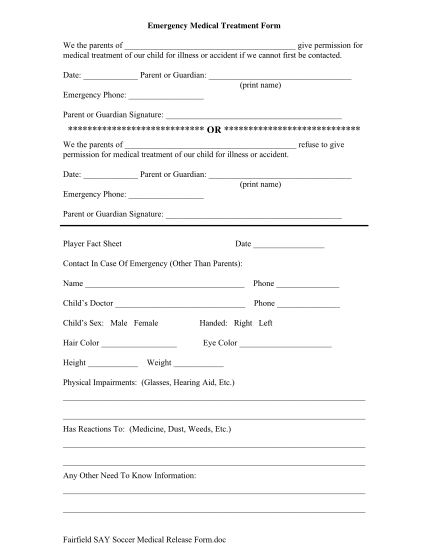
Medical Treatment Authorization bFormb - East Guernsey Local Schools - eguernsey k12 oh
East guernsey local schools medication/treatment administration at school dear parent: we receive many requests to administer medication and/or treatments during the school day. the following information is intended to clarify our policy on...
FILL NOW