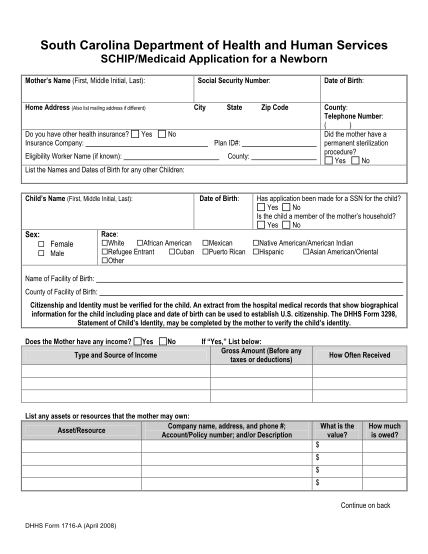
( Attachmt DHHS Form 1716-A SCHIP-Medicaid Application for a 205) - scdhhs
South carolina department of health and human services schip/medicaid application for a newborn mother s name (first, middle initial, last): social security number: home address (also list mailing address if different) do you have other health...
FILL NOW