- colorado
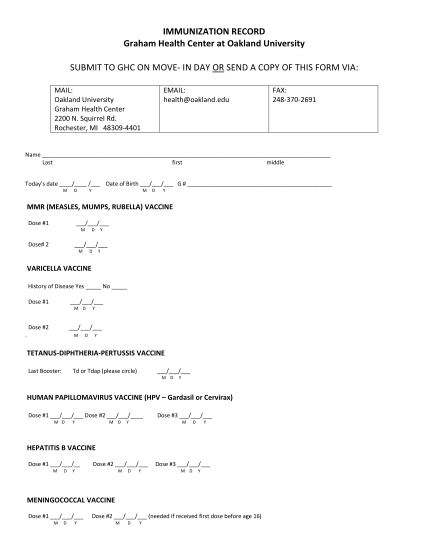
When do children and teens need vaccinations? please note: your child may need additional vaccines and possibly, less doses of the vaccines listed below depending on the type of vaccines that your healthcare provider uses. talk to your healthcare...
FILL NOW