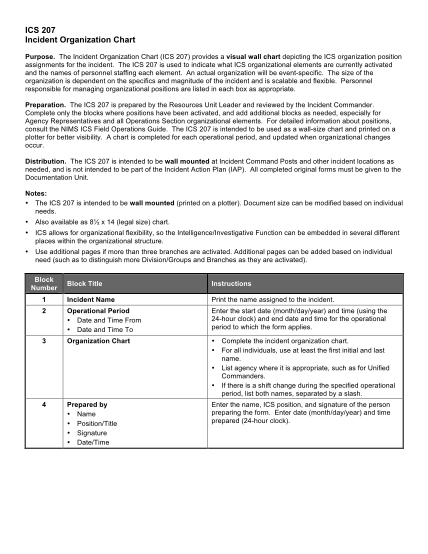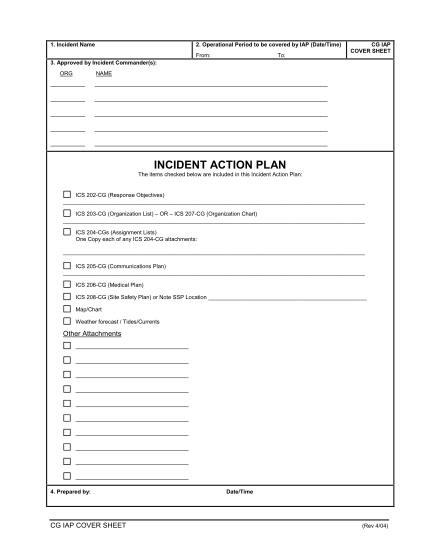
1 Incident Name 2 Operational Period to be covered by IAP
1. incident name 2. operational period to be covered by iap (date/time) from: to: cg iap cover sheet 3. approved by incident commander(s): org name incident action plan the items checked below are included in this incident action plan: ics 202cg...
FILL NOW