NAME DOA MG-Case ADDRESS MG Date PHONE CASE MANAGER HOME
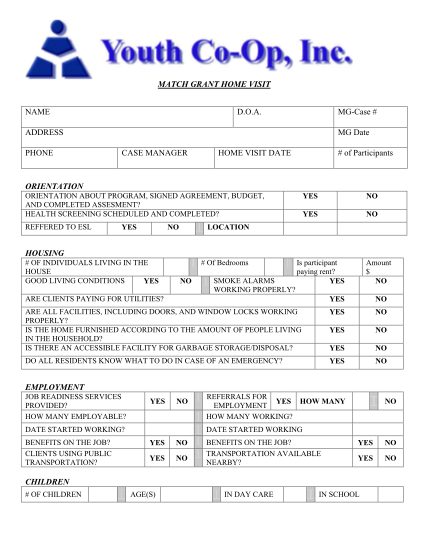
Match grant home visit name d.o.a. mgcase # address phone mg date case manager home visit date # of participants orientation orientation about program, signed agreement, budget, and completed assesment? health screening scheduled and completed?...
FILL NOW