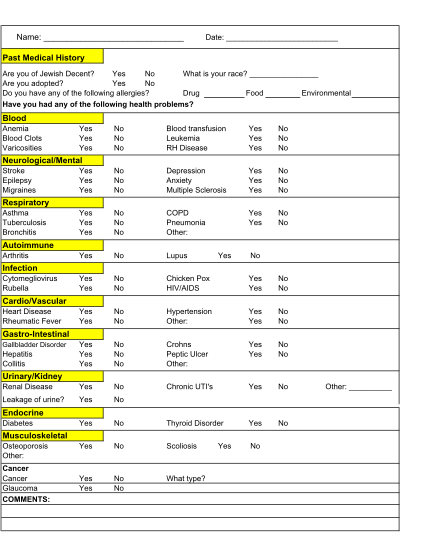
Name Date - Fairfax OB-GYN Associates
Name: date: past medical history are you of jewish decent? yes no what is your race? are you adopted? yes no do you have any of the following allergies? drug food environmental have you had any of the following health problems? blood anemia blood...
FILL NOW