AmeriCorps Application Cover Letter About AmeriCorps at ... - SLiCE - slice colostate
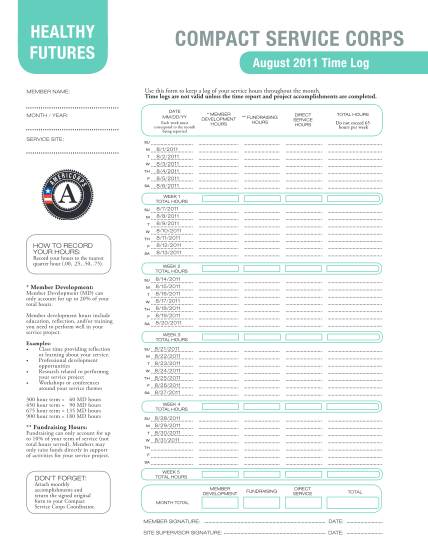
Healthy futures member name: compact service corps august 2011 time log use this form to keep a log of your service hours throughout the month. time logs are not valid unless the time report and project accomplishments are completed. date mm/dd/yy...
FILL NOW