23 Printable how to calculate resting heart rate Forms and Templates ...
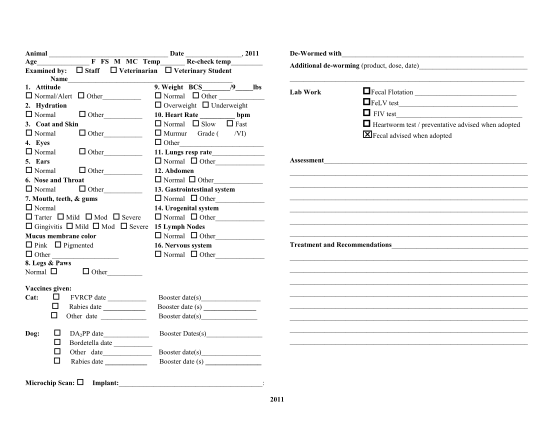
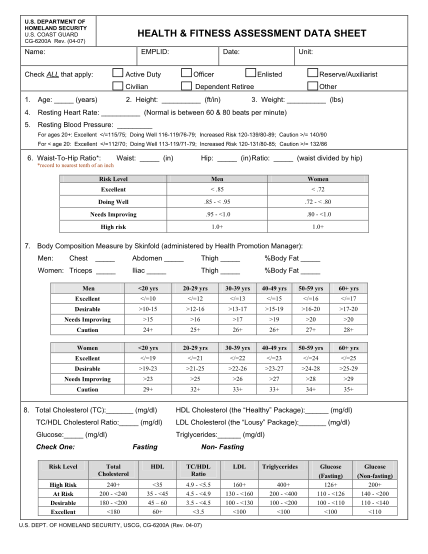
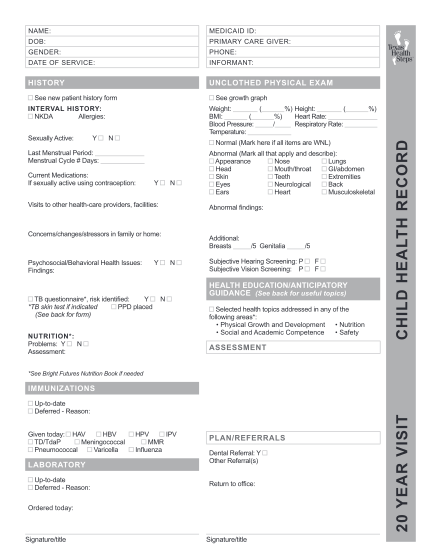
Name: medicaid id: dob: primary care giver: gender: phone: date of service: informant: history unclothed physical exam see growth graph sexually active: y %) height: ( weight: ( bmi: ( %) heart rate: blood pressure: / respiratory rate:...
FILL NOW