access to my chart at gillette specialty healthcare form
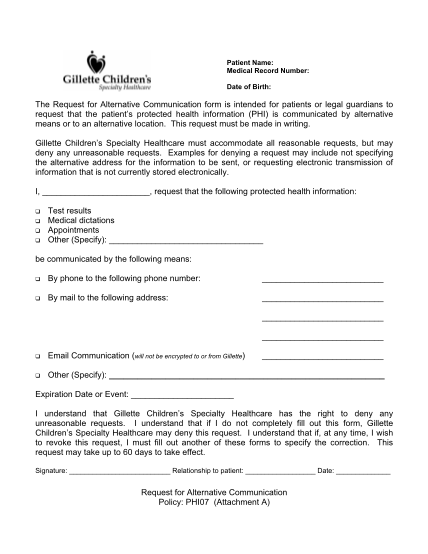
Patient name: medical record number: date of birth: the request for alternative communication form is intended for patients or legal guardians to request that the patient s protected health information (phi) is communicated by alternative means or...
FILL NOW