florida blue prior authorization form for medication
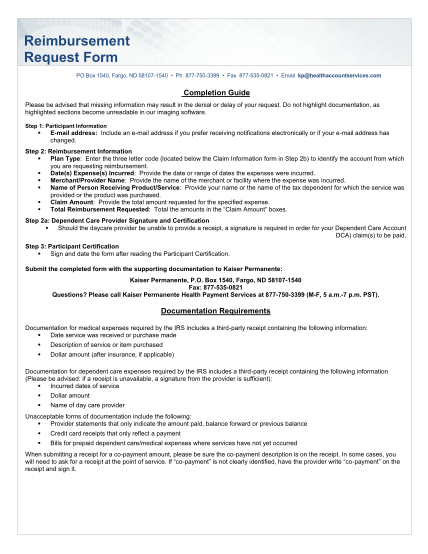
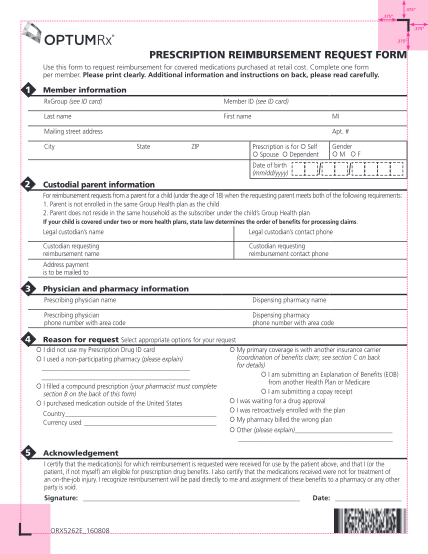
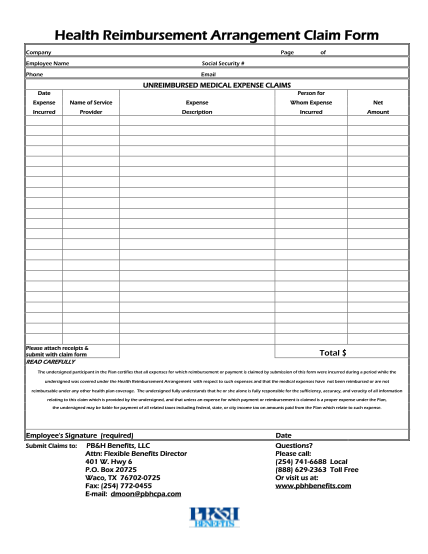
Prescription drug claim form directions: 1. complete and sign claim form below. use a separate form for each patient. 2. attach explanation of benefits (if applicable) and prescription receipts. 3. send completed form & pharmacy receipts to: prime...
FILL NOW