filled medical forms of troy university
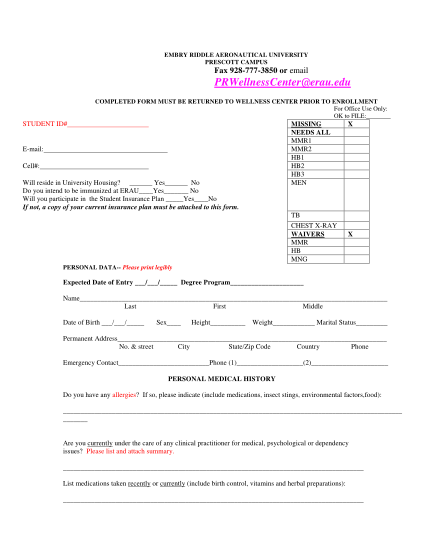
Embry riddle aeronautical university prescott campus fax 928--3850 or email prwellnesscenter erau.edu completed form must be returned to wellness center prior to enrollment for office use only: ok to file: student id# e-mail: cell#: will reside in...
FILL NOW