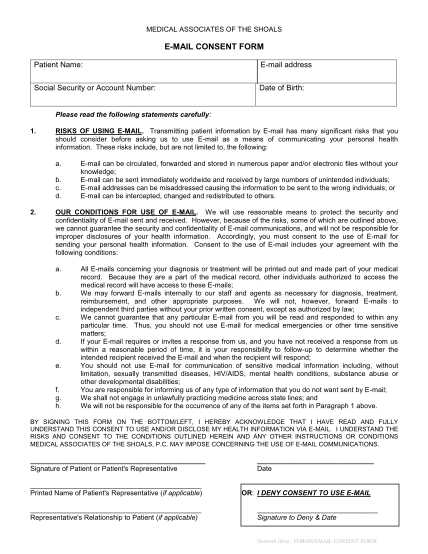
E-MAIL CONSENT FORM - Medical Associates of the Shoals
Medical associates of the shoals e-mail consent form patient name: e-mail address social security or account number: date of birth: please read the following statements carefully: 1. risks of using e-mail. transmitting patient information by...
FILL NOW