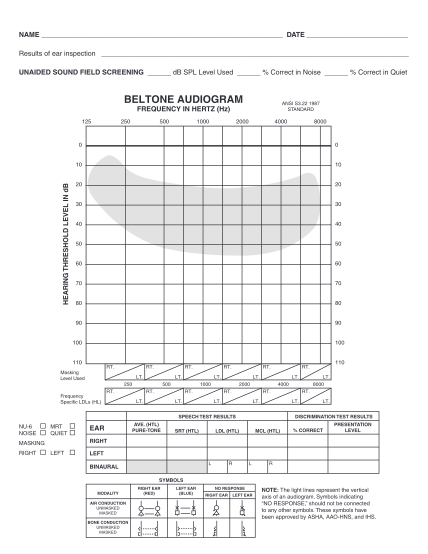
blank audiogram
Illinois department of public health in cooperation with date test number name (last) (first) (initial) birth date (month) / (day) / (year) parent/guardian (last) (first) grade phone ( ) address (number/street) (city) (zip code) testing location...
FILL NOW