Alabama Orthopaedic Clinic PC SPINE FORM Date Account
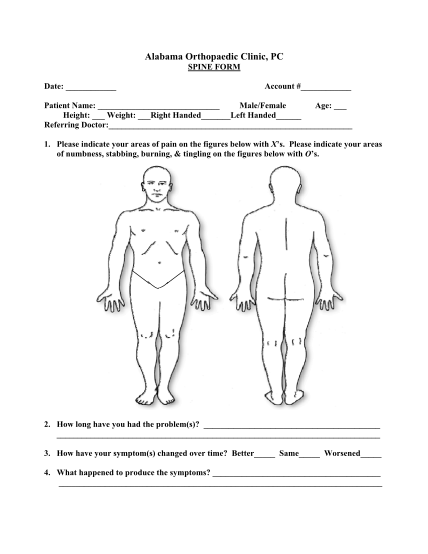
Alabama orthopaedic clinic, pc spine form date: account # patient name: male/female age: height: weight: right handed left handed referring doctor: 1. please indicate your areas of pain on the figures below with xs. please indicate your areas of...
FILL NOW