Authorization Form (.pdf) - myPHR
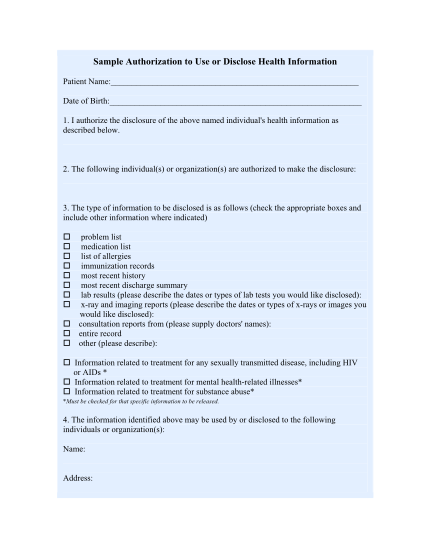
Sample authorization to use or disclose health information patient name: date of birth: 1. i authorize the disclosure of the above named individual's health information as described below. 2. the following individual(s) or organization(s) are...
FILL NOW