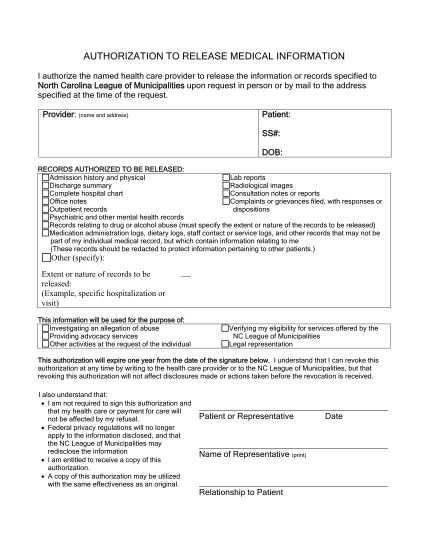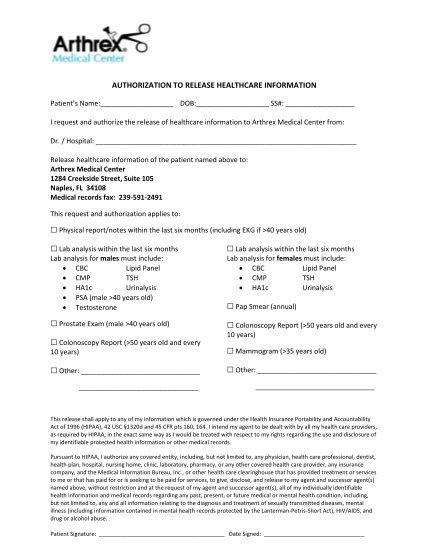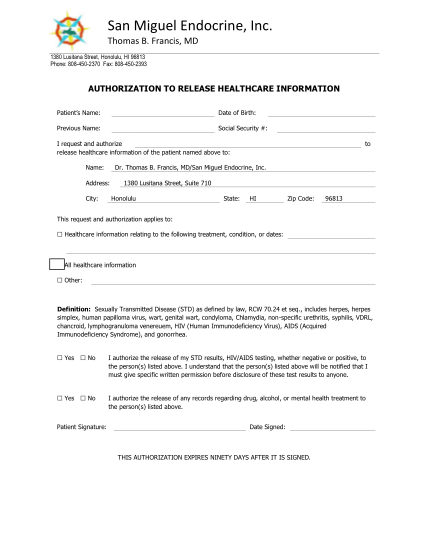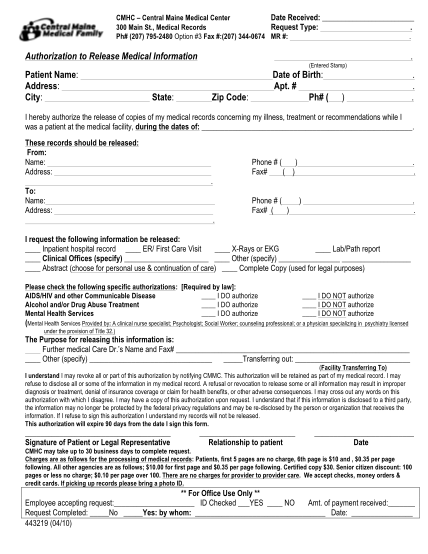
Authorization to release medical information from...
Authorization to release medical information from usmd uant i, , hereby authorize (name of patient or legal representative) uant (an affiliate of usmd affiliated services), to disclose the following information by q mail q fax q orally to: name:...
FILL NOW