Wv advance directive form fillable
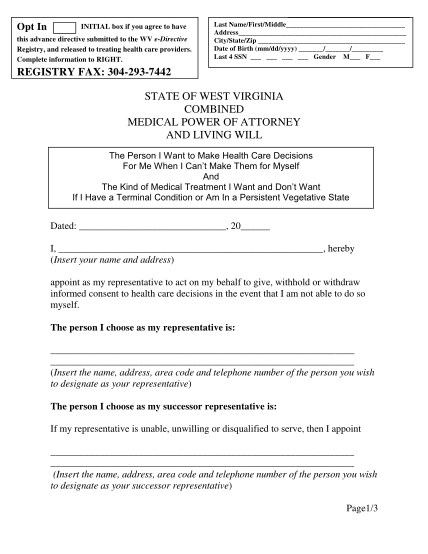
Opt in initial box if you agree to have this advance directive submitted to the wv e-directive registry, and released to treating health care providers. complete information to right. last name/first/middle address city/state/zip date of birth...
FILL NOW